


By LINDA BOYLE
The diagnosis of gender dysphoria in the U.S. has grown by leaps and bounds over the last ten to fifteen years. Data demonstrate increased prevalence among adolescents and young adults, with self‑reported transgender identity rising more rapidly in younger groups.
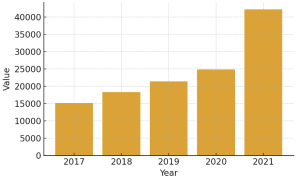
All but one of the 50 states saw an average increase in diagnoses of 96% from 2018-22. Virginia, Indiana, Utah and Alaska had the largest growth in diagnoses, ranging from 183% to 274%.

Youth make up approximately 18% of the transgender population.
President Trump signed Executive order 14187 on Jan. 28 requiring the Department of Health and Human Services to produce a report within 90 days on “the existing literature on best practices for promoting the health of children who assert gender dysphoria, rapid-onset gender dysphoria, or other identity-based confusion.”
HSS released an initial report in May and just released the final version on Nov. 19, entitled, “Treatment for Pediatric Gender Dysphoria Review of Evidence and Best Practices”.
HHS published this exhaustive peer-reviewed report that should make it clear to those who push “gender affirming care” on children that “the harms from sex-rejecting procedures — including puberty blockers, cross-sex hormones, and surgical operations — are significant, long term, and too often ignored or inadequately tracked.”
Within hours of the report being published, the American Academy of Pediatrics denounced it. Notably, the AAP statement cited no specific errors, only that the report “misrepresents the current medical consensus” and “prioritizes opinions over reviews of evidence.” Other medical associations followed suit.
Here are the findings and conclusions of the DHHS report:
- There is no compelling evidence for transitioning minors with gender dysphoria. The evidence that is available doesn’t give any clear benefit from using social transitioning, puberty blockers, cross-sex hormones, or gender modification surgery.
- However, there are substantial concerns about the potential harms from gender transition interventions to minors with gender dysphoria especially with puberty blockers, cross-sex hormones, and gender modification surgery. There is a lack of robust studies that have investigated these harms in the setting of gender transition in minors.
- The main Clinical Practice Guidelines for treating gender dysphoria in minors in the US are considered low quality. The World Professional Association for Transgender Health Standards of Care and Endocrine Society guidelines face issues such as conflicts of interest, flawed methods, and misrepresentation of evidence. (Add to this the WPATH isn’t even a medical scientific organization. It is an advocacy group.)
- Given the lack of demonstrable benefit and concern about potential harms, the use of puberty blockers, cross-sex hormones, and gender transition surgery in minors with gender dysphoria cannot be ethically justified.
The report stated that there are many risks associated with child sex changes to include “infertility, sexual dysfunction, impaired bone density accrual, surgical complications, and heart, metabolic, and psychiatric disorders — publication bias, a failure of existing studies to adequately track and report harms, and other factors may have obfuscated the true fallout of so-called “gender-affirming care.”
During the Biden years, the transgender Dr. Rachel Levine, Assistant Secretary for Health lobbied the WPATH to eliminate almost all minimum age restrictions for receiving this life altering medical and surgical interventions when WPATH published its recommendations. It happily bent the knee to Levine. Levine, who believes these surgeries are lifesaving, stated she was happy she didn’t transition in her teens years as she is glad she had children.
While many of the US medical associations denounced the HSS report, many European countries have already moved away from gender affirming care for minors citing the lack of compelling scientific evidence. The countries who have switched course include the UK, Sweden, Norway, Finland, and France. These countries now recommend a cautious approach that prioritizes psychological care as the first step in treatment.
French and Swedish health authorities have noted an increase in detransitions. French authorities warn of possible over-diagnosis, as clinicians cannot reliably predict which minors will outgrow gender dysphoria and which will not.
The American Medical Association and the American Academy of Pediatrics peddled the lie that chemical and surgical sex-rejecting procedures could be good for children,” HHS Secretary Kennedy said in a statement.
“They betrayed their oath to first do no harm, and their so-called ‘gender-affirming care’ has inflicted lasting physical and psychological damage on vulnerable young people,” continued Kennedy. “That is not medicine — it’s malpractice.”
Changes in reimbursements are coming based on this report. This is a billion dollar industry and creates customers for life.
Children who experience gender dysphoria deserve care to assist them. Many have made it to adulthood without being gender confused after completing their teen years.
These financial impacts to the medical community may be its greatest concern. Further research is needed before we permanently “convert” our children from the gender to which they were born.
But because there is such a huge fiscal impact to the medical community and big pharma, we can expect a huge push back and more misinformation.
Our children deserve better than this. Our children are precious and God’s gift.
They should not be viewed as a cash cow for the medical industry.
Linda Boyle, RN, MSN, DM, was formerly the chief nurse for the 3rd Medical Group, JBER, and was the interim director of the Alaska VA. Most recently, she served as Director for Central Alabama VA Healthcare System. She is the director of the Alaska Covid Alliance/Alaskans 4 Personal Freedom.
Linda Boyle: Medieval remedy may be first ‘new’ antibiotic in 40 years





One thought on “Linda Boyle: Federal report finds no evidence supporting gender transitions for minors, warns of significant harm”
I wonder if Part of the psychology kids suffering from growing up into their gender they were born if their dystopia started at home. Either they were afraid of the changes happening in their body, girls being uncomfortable by the puberty developing, or boys unsure of himself growing up into a man, or having parents who favored one gender over the other, or boys with bully controlling mothers who feminized her son by her controlling behavior
Just like suicide, gender dystopia, parents cant always blame schools and society without turning the mirror on themselves, “how did the parent contribute to their child’s self destruction (if the parent contributed anything at all)?
Because I’m honest and accountable. I grown up in Alaska to watch the suicide epidemic especially hitting GenZers hard when they were youth now GenAlphas, parents and family don’t look at themselves how they contributed. They don’t know when I look at those victims families I wouldn’t want to hang out with them because their family members are dysfunctional